Vitamin C, Cortisol and the Chemistry of Disease
A summary of Dr Thomas Levy’s recent presentation to our practitioner education group
I’ve followed Dr Thomas Levy’s work for years, and every time I sit down to listen to him I come away with another layer of nuance. His work has profoundly shaped the way I think about vitamin C, infection, toxins, dental pathology, inflammation and the chemistry of disease.
Recently, he presented to our practitioner education group on vitamin C, cortisol and the immune response. What follows is my summary of the key ideas he shared.
This article is not intended as a conventional consensus review. It is a presentation of Dr Levy’s redox model: his framework, his interpretation of the literature, and his clinical reasoning. Some of his positions are bold. Some challenge orthodox thinking. But that is precisely why his work is so valuable. He forces us to go back to first principles and ask what is actually happening inside the cell.
The central thread running through everything he teaches is deceptively simple:
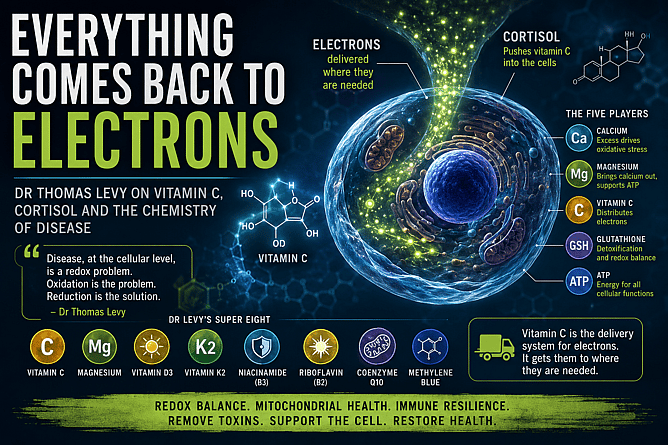
It all comes back to electrons.
The redox thesis
Dr Levy’s core argument is that disease, at the cellular level, is a redox problem. Reduction and oxidation are about electrons. Reduction means a molecule gains electrons. Oxidation means it loses them.
In Levy’s model, when a biomolecule loses electrons, it becomes oxidised and functionally impaired. Proteins, enzymes, lipids, membranes, mitochondria and DNA can all be affected. The result is not just “oxidative stress” as a side effect of disease. In Levy’s framework, the excess oxidation of intracellular biomolecules is the disease process itself.
This is one of his most important points.
He argues that there is no mysterious separate pathology inside a sick cell beyond the specific biomolecules that have been oxidised, how many are affected, where they are located, and how long they have remained in that oxidised state.
That is the lens he wants practitioners to use.
Instead of asking only, “What diagnosis does this person have?” we also need to ask:
What is oxidising the cell?
What toxins or infections are driving the electron loss?
What biomolecules are being damaged?
Is the cell able to restore its antioxidant capacity?
Can it still hold vitamin C, produce glutathione and make ATP?
This is why Levy uses the language of pro-oxidants and toxins almost interchangeably. In his model, a toxin is anything that takes electrons away from viable biomolecules. The damage caused by a toxin is the unique pattern of oxidation it leaves behind.
The counterpoint is the antioxidant. And for Levy, the prototype antioxidant — the master redox agent he returns to again and again — is vitamin C.
The five players inside the cell
Dr Levy frames intracellular oxidative stress around five interacting variables:
calcium, magnesium, vitamin C, glutathione and ATP.
These do not operate separately. They are dynamically connected.
His model runs roughly like this:
When intracellular calcium is high and magnesium is low, oxidative stress rises. As oxidative stress rises, vitamin C becomes depleted. Glutathione production drops because the enzymes that synthesise glutathione may themselves become oxidised and impaired. ATP production suffers because mitochondrial function becomes compromised.
This creates a vicious cycle.
High calcium drives oxidative stress.
Low magnesium permits calcium overload.
Low vitamin C weakens redox repair.
Low glutathione impairs detoxification.
Low ATP reduces the cell’s ability to restore order.
So, for Levy, a successful clinical protocol must not only “add antioxidants.” It must help restore the intracellular environment that allows the cell to hold vitamin C, rebuild glutathione and make ATP again.
That is why magnesium, vitamin C, mitochondrial support, toxin reduction and infection control are all central in his thinking.
Calcium: the marker and driver Levy says we have backwards
This is one of Levy’s most controversial and important areas of work, and it is the subject of his book Death by Calcium.
His view is that elevated intracellular calcium is both a marker and a driver of oxidative stress. In his words, if a cell is sick, intracellular calcium is elevated. The sicker the cell becomes, the higher calcium rises, right up to the point of apoptosis, necrosis or cell death.
This is why he is so strongly opposed to casual calcium supplementation.
Levy’s position is not simply that “too much calcium is bad.” His argument is that the modern obsession with calcium intake has missed the deeper issue: calcium belongs primarily in the bones and extracellular spaces, not accumulating inside cells and soft tissues where it can amplify oxidative stress and mitochondrial dysfunction.
From his perspective, increasing calcium intake without addressing magnesium, vitamin D, vitamin K2, mitochondrial function and redox status can push the body further in the wrong direction.
His conclusion is blunt: more calcium is not automatically better. In many cases, he believes it may be harmful.
The practical takeaway from his model is that we should stop thinking of calcium as a benign mineral that everyone needs more of. Calcium handling matters. Where calcium is located matters. And the intracellular calcium burden may be one of the most important markers of cellular stress.
Magnesium: the counterweight to calcium
If calcium wears the black hat in Levy’s model, magnesium wears the white one.
Levy describes magnesium as one of the most important tools we have for lowering intracellular calcium and improving cellular function. Magnesium acts as a natural calcium-channel blocker. It helps regulate calcium entry into the cell and supports the movement of calcium back out of the intracellular space.
In simple terms:
As magnesium comes in, calcium comes out.
That is the relationship Levy wants us to understand.
Magnesium is also essential for ATP biology. ATP is often described as the body’s energy currency, but biologically it is usually magnesium-ATP that is active. Without adequate magnesium, energy production, enzyme function, detoxification and electrical stability all suffer.
Levy also spoke strongly about magnesium and arrhythmias, sharing his own experience of resolving ectopic beats with sustained high-dose liposomal magnesium and IV magnesium. His position is that many rhythm disturbances reflect inadequate intracellular or mitochondrial magnesium, even when standard serum magnesium appears normal.
This is an important clinical point. Serum magnesium can look normal while intracellular magnesium is still inadequate. Levy’s broader message is that magnesium is often under-dosed, under-tested and under-appreciated.
Vitamin C as an electron distributor
One of the most fascinating parts of Levy’s presentation was his updated thinking on vitamin C.
The conventional view is that vitamin C works because it donates electrons. Levy still accepts that vitamin C participates in electron donation, but he now believes its primary role is even more elegant:
Vitamin C distributes electrons through the body.
He used the analogy of a factory producing thousands of widgets but having only two delivery trucks. The widgets are electrons. The trucks are vitamin C. If you do not have enough trucks, the widgets cannot get where they need to go.
In this model, food supplies the body with large amounts of new electrons. Vitamin C helps distribute those electrons. It cycles between reduced ascorbate and oxidised dehydroascorbic acid, moving through tissues, entering cells, being recycled, and helping restore oxidised biomolecules.
This is why Levy does not view oxidised vitamin C as useless. Dehydroascorbic acid has no electrons left to donate in that moment, yet it can still enter cells and be reduced back to ascorbate. Levy points to this as evidence that vitamin C is not merely an electron donor but part of a much larger electron transport and distribution network.
That is a profound reframe.
It also helps explain why vitamin C status can be so central in infection, toxin exposure, inflammation and mitochondrial dysfunction. If vitamin C is depleted, the body may still have electrons available from diet and metabolism, but it loses part of its delivery system.
Cortisol pushes vitamin C into the cell
Levy then tied vitamin C to cortisol in a way many practitioners have not fully appreciated.
Cortisol is usually described as an anti-inflammatory hormone. But Levy’s argument is that cortisol’s anti-inflammatory effect is deeply connected to vitamin C.
His mechanism is this: cortisol enters the cell, binds to its receptor, and the receptor complex moves to the nucleus. This then increases expression of vitamin C transporter proteins on the cell membrane, increasing the cell’s ability to take up vitamin C.
In Levy’s words:
Cortisol pushes vitamin C into the cells.
That is the key sentence.
From his perspective, cortisol is not simply “suppressing inflammation.” It is helping deliver the molecule that can restore redox balance inside the inflamed cell.
This is also why he distinguishes sharply between natural cortisol, also known as hydrocortisone when prescribed, and synthetic corticosteroids like prednisone or dexamethasone. Levy’s position is that hydrocortisone, used properly, can be a physiological replacement of a deficiency, whereas synthetic corticosteroids are pharmacological drugs with a very different risk profile.
He is especially concerned that many people today are not only vitamin C deficient but also functionally adrenally insufficient. In other words, when infection or toxic stress hits, they may not produce enough cortisol to move vitamin C into cells effectively.
In Levy’s model, this is one reason people become vulnerable to infections. It is not only the pathogen. It is the terrain: low vitamin C, inadequate cortisol response, poor intracellular redox status and weakened immune capacity.
Vitamin C, cortisol and infection
This is where Levy’s work becomes most clinically provocative.
He argues that when an acute infection begins, the body should mount a coordinated response: cortisol rises, vitamin C should be mobilised, immune cells become activated, and vitamin C is pushed into the tissues where it is needed.
Animals that make their own vitamin C can increase vitamin C production under stress. Humans, guinea pigs, fruit bats and primates cannot make vitamin C in the same way, so we depend on dietary and supplemental intake.
Levy’s point is that in humans, cortisol may rise during stress, but if vitamin C is not available in sufficient amounts, the cortisol cannot do its full job. It is trying to push vitamin C into cells, but there may not be enough vitamin C to push.
This is why he believes vitamin C and hydrocortisone belong together in certain acute settings, especially early infection. His argument is that vitamin C provides the redox support, while cortisol helps deliver it intracellularly.
He is careful to distinguish early infection from very advanced critical illness. His view is that the earlier the combination is used, the more powerful it may be. Once severe sepsis is advanced, the physiology is much more oxidised, receptors may be impaired, and the situation becomes harder to reverse.
This is not a casual self-treatment recommendation. Hydrocortisone is prescription-only and should be used under appropriate clinical supervision. But Levy’s mechanistic argument is important: in his model, infection is not only about killing pathogens. It is about restoring redox balance inside cells under acute oxidative attack.
The immune system as a vitamin C delivery service
Levy’s reframe of immunology is simple and memorable.
In his model:
Inflammation means local vitamin C depletion.
Local vitamin C depletion means inflammation.
He argues that these are two ways of describing the same physiology.
When tissue becomes inflamed, the immune system sends in first responders. One of the key early immune cells is the monocyte. Levy emphasises that monocytes and other leukocytes concentrate vitamin C at levels far higher than plasma.
This leads to one of his most elegant ideas:
The immune system is, in part, a vitamin C delivery system.
The inflamed tissue has used up its vitamin C. The immune cells arrive loaded with vitamin C, magnesium and hydrogen peroxide. They help restore vitamin C to the depleted area while also participating in pathogen killing.
Levy also discussed the role of vitamin C, hydrogen peroxide and iron chemistry in generating hydroxyl radicals inside infected cells or around pathogens. This is one of the paradoxes of vitamin C: in the right context, it can support antioxidant protection, but in the presence of catalytic metals and peroxide it can also help generate highly reactive species that damage pathogens or infected cells.
That is why Levy sees vitamin C as both protective and antimicrobial, depending on the biochemical environment.
Again, the key is context. Vitamin C is not just “an antioxidant.” It is a redox-active molecule involved in electron movement, immune cell function, pathogen response and tissue repair.
Toxins, infections and dental pathology
Another major part of Levy’s model is that toxins and infections drive oxidative stress.
He defines a toxin as anything that pulls electrons away from biomolecules. Infections do this through their metabolic by-products, inflammatory activation, free iron release and tissue damage.
This is why Levy has written so extensively about hidden infections, especially dental infections. He considers chronic dental pathology, including infected root canals and jawbone cavitations, to be one of the most overlooked drivers of systemic oxidative stress.
His position is that focal infections can quietly produce ongoing pro-oxidant burden for years. A person may not feel pain, and a standard dental X-ray may look normal, yet a cone-beam CT can reveal deeper pathology.
This was personally relevant to me. After learning from Levy’s work, I pursued cone-beam imaging and discovered significant dental issues that had not been obvious on standard assessment. That experience changed the way I think about hidden sources of inflammation and oxidative burden.
Whether we are talking about dental infections, gut pathogens, heavy metals, iron overload, environmental toxins or chronic inflammatory triggers, Levy’s question is the same:
What is oxidising the system, and how do we remove or neutralise it?
Vitamin C and toxin neutralisation
Levy has long argued that vitamin C is one of the most powerful anti-toxin agents available.
His reasoning follows directly from his redox model. If a toxin causes harm by oxidising biomolecules, then a sufficiently available antioxidant can help neutralise that oxidative effect by donating or distributing electrons.
He has written about vitamin C in relation to many forms of toxic exposure, including heavy metals, venom, pesticides, alcohol and drug toxicity. His view is that vitamin C, properly dosed and delivered, can chemically satisfy electron-seeking toxins and reduce the damage they do to tissues.
This is one reason he is such a strong advocate for high-dose vitamin C, including intravenous vitamin C where appropriate, and liposomal vitamin C where IV access is not available.
The key phrase here is “properly dosed and delivered.” Levy repeatedly emphasises that tiny doses are often not enough for serious oxidative stress. His view is that dose matters enormously.
The insulin, glucose and vitamin C connection
Levy also introduced a more speculative but fascinating idea around insulin, glucose and vitamin C.
Most animals make vitamin C from glucose in the liver. Humans have lost that ability. Levy argues that this has major metabolic consequences.
In animals that produce vitamin C, glucose can be diverted into vitamin C synthesis during stress. In humans, that pathway is not available, so glucose accumulates and must be handled differently. Levy suggests that insulin may be more deeply connected to vitamin C transport than is commonly appreciated.
His hypothesis is that one of insulin’s most important roles may be facilitating cellular uptake of vitamin C, not merely glucose. In this view, the modern diabetes problem may be linked, at least in part, to our lost ability to convert glucose into vitamin C under stress.
This is not conventional biochemistry textbook teaching, and Levy presents it as his own evolving hypothesis. But it is a provocative idea that fits within his broader redox framework.
If stress should trigger both cortisol and vitamin C mobilisation, and humans cannot make vitamin C, then our stress response may be incomplete unless vitamin C is supplied externally.
Levy’s practical “super eight”
Dr Levy closed with what he calls his “super eight” supplements:
Vitamin C
Magnesium
Vitamin D3
Vitamin K2
Niacinamide
Riboflavin
Coenzyme Q10
Methylene blue
The first four he frames around lowering intracellular calcium, improving redox balance and supporting immune function. The second four he connects to ATP production and the electron transport chain.
Niacinamide is especially important in his model because it is a direct precursor to NAD, which is central to mitochondrial energy production and electron transfer. Levy’s position is that niacinamide is a much cheaper and more direct way to support NAD biology than expensive NAD infusions.
Riboflavin supports flavoproteins and mitochondrial energy pathways. CoQ10 participates directly in the electron transport chain. Methylene blue, in Levy’s view, is one of the most powerful redox-active compounds available and may support electron flow in compromised mitochondria.
This is not meant as a one-size-fits-all prescription. Dosing, contraindications, medications, genetics, kidney function, iron status and individual tolerance all matter. Methylene blue in particular requires care because of drug interactions and contraindications.
But as a framework, Levy’s “super eight” is coherent. It is built around the same core goal:
Restore vitamin C.
Lower pathological intracellular calcium.
Increase magnesium.
Support glutathione.
Improve ATP production.
Reduce oxidative stress.
My take
What I love about Levy’s work is that he brings us back to first principles.
He is not asking us to memorise another complex disease pathway. He is asking us to look at the chemistry underneath the pathology.
Where are electrons being lost?
What is oxidising the cell?
Is calcium accumulating where it should not?
Is magnesium sufficient?
Is vitamin C available and able to enter the cell?
Can glutathione be produced?
Can mitochondria make ATP?
Are infections, toxins, dental pathology, iron, gut issues or hormone deficiencies driving the oxidative burden?
That is a powerful way to think.
Some of Levy’s conclusions challenge mainstream medicine. That does not make them wrong. Many important medical advances began as challenges to consensus. But it does mean we need to be precise in how we present them.
This is Dr Levy’s model. It is a redox model of disease. It places vitamin C, magnesium, cortisol, mitochondrial function and toxin removal at the centre of clinical thinking.
And whether one agrees with every detail or not, the core message is hard to ignore:
The cell runs on electrons.
Disease reflects electron loss.
Healing requires restoring redox balance.
Everything comes back to electrons.